Retinopathy of prematurity (ROP) is a common and serious eye condition affecting premature infants. It occurs when the blood vessels in the retina develop abnormally, potentially leading to vision impairment or even permanent blindness if not detected and treated promptly. This article provides detailed information on the causes, symptoms, treatment options, and prevention methods for ROP, helping parents understand essential factors to protect their child’s eye health.
What is Retinopathy of Prematurity (ROP)?
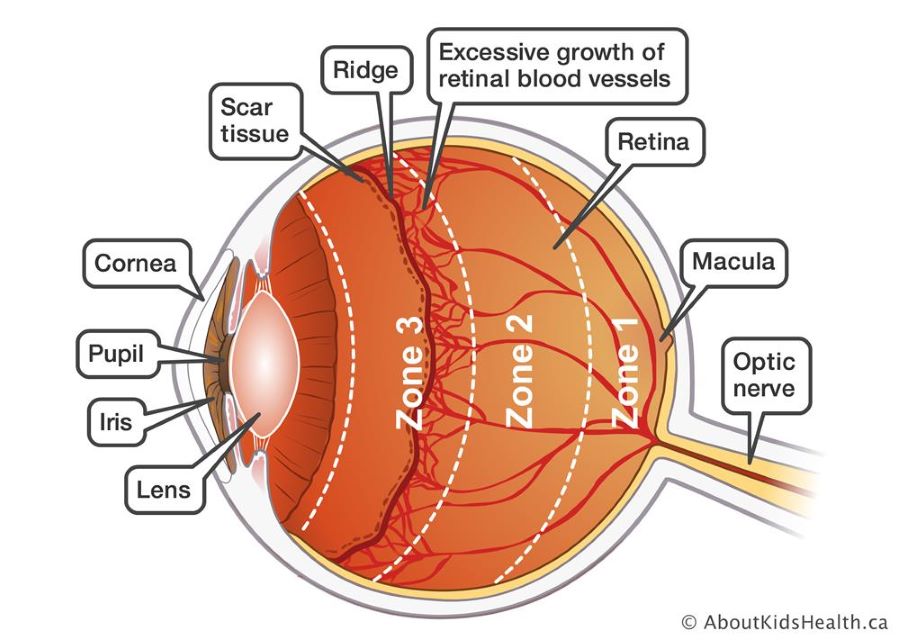
Retinopathy of prematurity (ROP) is a pathological condition occurring in preterm infants, especially those born before 32 weeks of gestation. In these infants, the retinal blood vessels, which normally develop late in pregnancy, fail to mature properly. Premature birth disrupts the normal vascular growth in the retina, causing abnormal blood vessel formation. These abnormal vessels can leak, scar, or detach the retina, leading to visual impairment.
If left undiagnosed or untreated, ROP may cause severe eye complications ranging from reduced vision to permanent blindness. Early detection and timely treatment are critical to preserving vision in affected infants.
For premature infants, treating and monitoring conditions like ROP requires a close combination of early diagnosis and effective treatment solutions for pediatric eye diseases.
Causes of Retinopathy of Prematurity (ROP) in Preterm Infants
Retinopathy of prematurity (ROP) primarily occurs due to abnormal development of the retinal blood vessels in premature infants whose bodies and organs have not fully matured. Key causes include:
- Premature birth: Infants born before 32 weeks of gestation have a higher risk of ROP because their retinal blood vessels are underdeveloped.
- Inadequate oxygen supply: Preterm infants often require oxygen therapy to sustain life. However, improper or sudden changes in oxygen delivery can increase the risk of abnormal blood vessel growth in the retina.
- Low birth weight: Infants weighing less than 1.5 kg at birth have a higher risk due to incomplete development of organs and blood vessels.
- Prolonged oxygen therapy: Extended use of oxygen support may increase the likelihood of developing ROP. Both insufficient and excessive oxygen can damage the retinal vessels.
- Infections and genetic factors: Although less common, certain infections or genetic predispositions may contribute to the development of ROP.
Understanding these causes helps parents and healthcare providers implement timely prevention and treatment strategies to protect the child’s vision.
Symptoms of Retinopathy of Prematurity (ROP) in Preterm Infants
ROP often has no obvious symptoms in its early stages, making regular eye examinations critical for early detection. As the disease progresses, some signs may include:
- Reduced or lost vision: Infants may not respond to moving objects or light, or have difficulty seeing distant objects.
- Abnormal eye movements: In severe cases, infants might show unusual eye movement patterns or prefer to look in one direction.
- Abnormal eye size: Some infants may have eyes that appear larger or smaller than normal.
- Redness or light sensitivity: The eyes may appear red or swollen, indicating abnormal retinal changes.
- Abnormal light reflex: Infants may not blink or respond normally to bright light.
Because early symptoms can be subtle or absent, it is essential for parents to ensure preterm infants undergo regular eye screenings to detect ROP early and initiate prompt treatment.
Treatment Methods for Retinopathy of Prematurity (ROP) in Preterm Infants
If not detected and treated early, retinopathy of prematurity (ROP) can lead to severe vision problems or permanent blindness. However, with timely diagnosis, effective treatments can help prevent or reduce damage. The main treatment methods include:
Regular monitoring
For preterm infants at risk of mild ROP, doctors closely monitor retinal blood vessel development through scheduled eye exams. This allows early detection and timely intervention.
Laser therapy
The most common treatment for ROP. Laser therapy stops the abnormal growth of retinal blood vessels by using a focused laser beam to destroy these vessels, preventing further damage and helping to preserve vision.
Surgical treatment
In severe cases where there is a risk of retinal detachment, surgery may be needed. Surgery aims to remove or repair damaged tissues in the eye to prevent vision loss.
Anti-VEGF injections
In some cases, doctors inject medications into the eye to inhibit abnormal blood vessel growth. These injections reduce retinal damage risk and help protect vision.
Supportive care
Ensuring overall health through adequate oxygen supply, proper nutrition, and maintaining a healthy weight also plays a crucial role in reducing ROP risk and improving treatment outcomes.
Early detection and appropriate treatment are essential to protect vision, minimize blindness risk, and improve the child’s quality of life.
>> In severe cases of ROP that do not respond to laser or medication treatment, retinal detachment surgery may be necessary to preserve vision.

Prevention of Retinopathy of Prematurity (ROP) in Preterm Infants
Preventing ROP is critical, especially for preterm infants at high risk. Effective prevention strategies include:
- Close prenatal care: Pregnant women should have regular health check-ups and follow medical advice to avoid premature birth. A healthy pregnancy reduces the risk of prematurity and subsequently ROP.
- Proper neonatal care environment: Preterm infants require specialized care during their first weeks. Maintaining optimal temperature, humidity, and oxygen levels helps reduce ROP risk. Close monitoring by pediatric specialists is essential.
- Regular eye screenings: Preterm infants need early and frequent eye exams to detect ROP before symptoms appear. Early diagnosis allows timely treatment to prevent progression.
- Careful oxygen management: Oxygen therapy must be precisely controlled to avoid too much or too little oxygen, both of which increase ROP risk. Medical staff should monitor oxygen saturation levels carefully.
- Adequate nutrition: Proper nutrition, especially sufficient intake of vitamins A and D, supports eye and overall development, reducing susceptibility to retinal diseases.
- Minimizing exposure to intense light: Protecting preterm infants from strong or direct light helps prevent retinal damage.
Implementing these preventive measures helps safeguard the eye health of preterm infants, reducing ROP incidence and supporting normal vision development.
Retinopathy of prematurity (ROP) is a serious condition that can impact the long-term vision of infants born before 32 weeks. However, with careful monitoring, timely treatment, and preventive care, the risks can be significantly reduced. Close cooperation between healthcare providers and families is key to giving children the best chance for healthy vision development.